What to Tell Your Doctor About Your Gut Symptoms (So the Appointment Isn't a Waste)
I'd spent two years trying to figure out what was going on with my gut when I got yet another appointment with a gastroenterologist. I remember sitting down in her office and immediately starting to describe gut symptoms to the doctor from memory. Two years of symptoms. In fifteen minutes. Starting from the beginning.
She was kind. She listened. At the end, she handed me a low FODMAP handout and booked a follow-up for three months later.
I left with nothing new.
That appointment failed because I had no idea how to present what I knew in a way that was actually useful. Not because she wasn't good at her job. This changed when I started bringing a structured symptom history instead of a verbal summary. This is what that looks like, and why it matters so much more than I thought.

Why Appointments Feel Like a Waste (and Why It's Not Actually the Doctor's Fault)
Doctors work from pattern recognition. They're scanning for clusters of information that point toward a root cause: timing, how symptoms have changed over time, what's been tried, what helped even slightly. The pattern only becomes visible when the data is organized.
Fifteen minutes is actually enough time, if the information is in the right format. Most people walk in with a verbal summary across years of memory, and that's genuinely hard to work with, for everyone in the room.
When you're describing symptoms from memory, you skip context without realizing it. "I've had bloating for about two years" leaves out that it got significantly worse after a stomach infection, that it correlates with stress, and that low FODMAP helped for a while before stopping. That context is what makes patterns visible. Without it, the doctor has a description with nothing to anchor it to.
⚠️ Saying "I've always had a sensitive stomach" tells a doctor almost nothing. The details that feel minor to you (when it changed, what you'd been eating, what you'd just tried) are often the most useful data points.
What Actually Changed When I Came Prepared
The night before another appointment, I spent a couple of hours putting together a written history. When symptoms started, what had changed over time, everything I'd tried in rough chronological order, what had actually made any difference. I emailed it to the clinic the day before.
The doctor actually reviewed the history prior to the appointment, and her questions were way more specific and straight to the point. We weren't circling around low FODMAP anymore, we were discussing angles that I haven't yet explored (and I figured the root cause was in the upper GI in my case, even if the main symptoms were downstream in the gut)
💡 Sharing your symptom history in writing before the appointment (even just as an email attachment) means the doctor can review it on their own time. The fifteen minutes becomes actual conversation instead of history-taking.
Dr. Megan Riehl, a GI health psychologist at Michigan Medicine, has focused her work on exactly this intersection. When a practitioner already has organized data, the appointment shifts from collection to interpretation.
The appointment is essentially a data transfer. Once I understood that, I stopped trying to explain everything from scratch and started thinking about how to present it.
What a Complete Gut History Actually Looks Like
This is the practical part. A structured gut history doesn't need to be long or formal. It needs the right information in a format a doctor can scan in about two minutes.
Here's what to include:
- Start with when symptoms started and whether there was a clear trigger (an infection, an antibiotic course, a period of sustained stress, a diet change). Note how things have changed since then (better, worse, different pattern).
- Use the Bristol Stool Chart to describe your stool pattern: it rates stool type from 1 (hard lumps) to 7 (fully liquid). "Mostly type 6, sometimes type 1, frequency varies between 3 times a day and once every two days" gives a practitioner far more to work with than "it varies."
- Triggers beyond food. Stress, sleep quality, hormones (particularly menstrual cycle timing), physical activity, medications. All of these affect gut function. The gut-brain axis is real. Multiple meta-analyses have confirmed that psychological stress reliably worsens symptom severity in IBS, with the effect documented across both pain and bowel habit disruption (source: Gut, 2019; Alimentary Pharmacology and Therapeutics, 2020).
- Everything you've tried, with rough dates and outcomes. "Low FODMAP for 8 weeks: bloating improved, pain unchanged." "Probiotic X for one month: no noticeable effect." This tells a doctor what's been ruled out and what might be worth revisiting.
- And state any red flags directly: blood in stool, unexplained weight loss, symptoms waking you at night, family history of IBD or colorectal cancer. Don't bury these.
⚠️ Don't just list supplements you've taken. Note the dose, how long you took it, and what actually happened. "I tried probiotics" gives a doctor almost nothing. Specific outcomes are what create useful data.
A list or simple table is easier for a doctor to scan than a paragraph of prose. Think of it as something they'll look at for 90 seconds before walking in, not a document they'll read carefully. Just look at this:
| Information | Vague version | Useful version |
|---|---|---|
| Stool pattern | "It varies" | "Bristol type 5-6, 3x daily, worse in the morning" |
| What you've tried | "I've tried probiotics" | "Florastor 2x daily, 6 weeks, urgency slightly better, bloating unchanged" |
| Triggers | "Stress, probably" | "Symptom flares reliably after 3+ nights of poor sleep" |
| Timeline | "It's been bad for a while" | "Significant worsening after stomach bug in March 2023" |
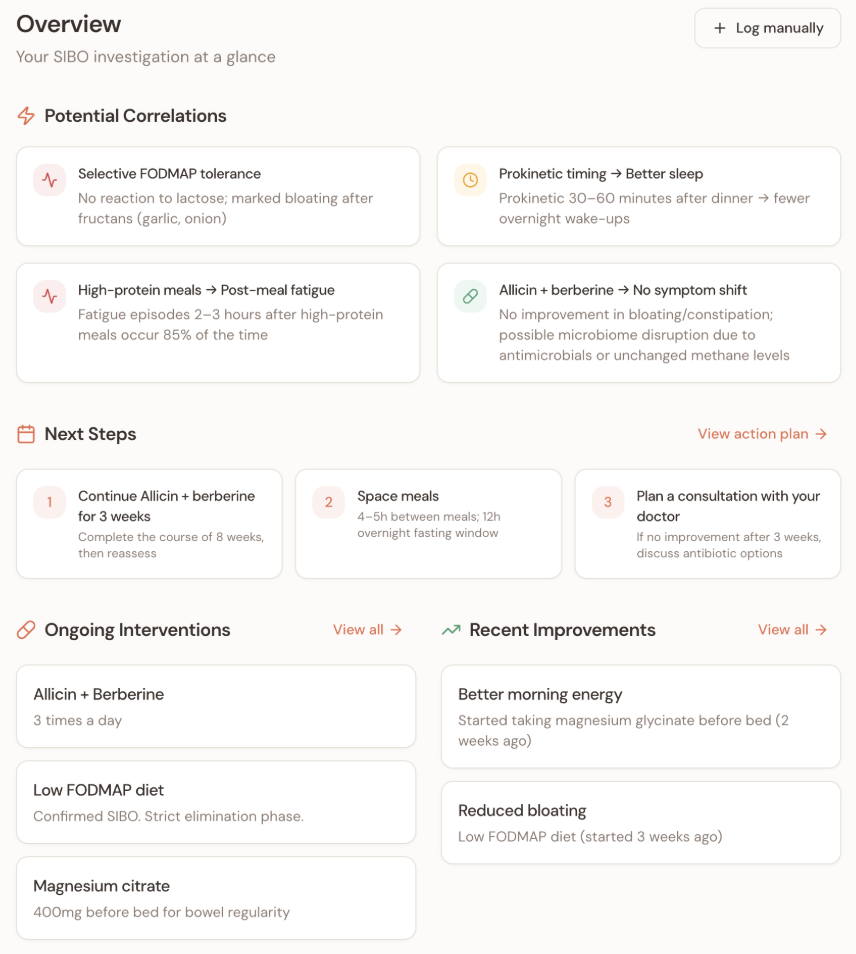
Building this kind of history from scratch takes a few hours if you're doing it manually. Noorish does it automatically. The free gut health audit walks you through your symptom history and generates an organized record you can share with a practitioner before an appointment, so you don't have to start from a blank page.
🔎 If you want an organized symptom history without building it manually: Noorish builds a structured gut health record from your full history, so the conversation starts from data rather than memory. Start here →
[Noorish screenshot here]
If Your GP Has Never Heard of SIBO
This comes up a lot. A GP who isn't familiar with small intestinal bacterial overgrowth won't know what to test for, what to look for, or where to send you.
Bringing a one-page summary of what SIBO is (from Mayo Clinic or a gastroenterology association) can frame the conversation without it feeling confrontational. It shows you've done research, not that you've self-diagnosed.
SIBO sits in a gap between primary and specialist care. Most GPs weren't trained in breath testing or functional GI conditions in any depth, and familiarity varies a lot depending on where you are and who you see. That's not a criticism. It's just useful context for framing the conversation.
Conclusion
The appointment was a waste because the information wasn't in the right format. That's a fixable part.
When you come in with organized data, the conversation shifts to what to do next rather than re-establishing what happened. That's where having a structured record matters. Noorish turns your symptom history into a document you can share with a practitioner before an appointment, so your next one starts from data instead of memory. If you're at the stage of trying to get more out of medical appointments, it's worth a look.
🔎 Noorish: Gut Health Action Plan
Walk into your next appointment with organized data instead of two years of symptoms from memory.
- ✅ Build a structured gut symptom history to share with your doctor
- ✅ Understand what's actually driving your symptoms
- ✅ Get a science-based action plan for what to try next
- ✅ Optional: validation from a real nutritionist
FAQ
What should I tell my doctor about gut problems?
The most useful things to bring are a symptom timeline (when it started and how it's changed), your stool pattern using the Bristol Stool Chart as a reference, a list of what you've tried with rough dates and outcomes, and any triggers you've noticed beyond food. Presenting this in writing before the appointment, rather than verbally in the room, gives the doctor time to review the data before you sit down.
How do you describe abdominal pain to a doctor?
Be specific about location (upper, lower, left, right, or diffuse), timing (constant vs. comes and goes, better or worse after eating, related to bowel movements), and severity on a 1-10 scale. Note what makes it better or worse. Also note whether it wakes you from sleep (nocturnal pain is a red flag that changes the clinical picture).
What questions will a gastroenterologist ask me at my first appointment?
Expect questions about when symptoms started, whether there was a trigger event, your stool pattern, what makes symptoms better or worse, what you've tried, and whether there's any family history of GI conditions like IBD or colorectal cancer. Having this information organized before you go means you can answer precisely instead of guessing from memory.
What is the most important information to bring to an IBS appointment?
A symptom timeline (when it started, how it's changed), a stool pattern log using the Bristol Stool Chart, a clear list of what's been tried and what happened, and your known triggers. If you've tracked symptoms, bring that data. The goal is to give the doctor enough organized information to identify patterns in two minutes of review rather than fifteen minutes of questions.
How do I explain SIBO to a doctor who isn't familiar with it?
Frame it as a question rather than a conclusion: "I've been reading about small intestinal bacterial overgrowth as a possible explanation for some of my symptoms. Can we discuss whether a breath test would be appropriate?" Bringing a one-page summary from a reputable source (Mayo Clinic, a gastroenterology association) can help frame the conversation. Ask specifically about a lactulose or glucose breath test, or a referral to a gastroenterologist who works with functional GI conditions.